| Content note: This article includes clinical language about the pelvic floor (including vagina, anus, urination, bowel movements, sex, and sexual trauma). Please skip around as needed and take care of yourself. |
Is My Pelvic Floor Weak… or Just Tight?”
If you’ve been told your pelvic floor is “weak,” you are not alone.
It’s the default explanation for everything: leaking when you sneeze, pelvic floor pain, painful sex, constipation, frequent urination, postpartum heaviness, hip tightness, low back pain… all of it gets lumped into one big bucket called “weak pelvic floor.”
But here’s the plot twist that’s leaving a lot of women frustrated (and sore):
Many women who are told their pelvic floor is weak actually have a pelvic floor that’s too tight. And yes, you can also be both weak and tight at the same time.
This is why women end up stuck in the cycle of:
- Googling “pelvic floor won’t relax”
- Doing more Kegels
- Feeling worse
- Thinking something is wrong with them
Nothing is wrong with you. Your body is patterned. And your pelvic floor is often acting like a tiny nervous system “first responder.”

Is My Pelvic Floor Weak… or Just Tight?”
Let’s start with the most important reframe:
Your pelvic floor isn’t binary. It’s not like:
- weak = bad
- strong = good
It’s more like a set of pelvic floor muscles (plus fascia + nerves + breath pressure) that need range.
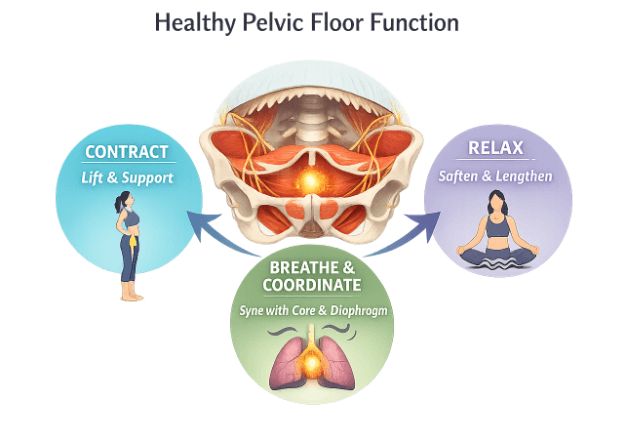
A healthy pelvic floor can:
- contract (lift and support)
- relax (soften and lengthen)
- coordinate with your breath and your deep core
When that coordination gets disrupted, we land in the world of pelvic floor dysfunction.
Misdiagnosis happens because we’re living in a culture that equates “fixing” with “strengthening.”
The Pelvic Floor Is Not Just “Strong or Weak” — It’s a Nervous System
Understanding how the pelvic floor functions can be the first step to healing.
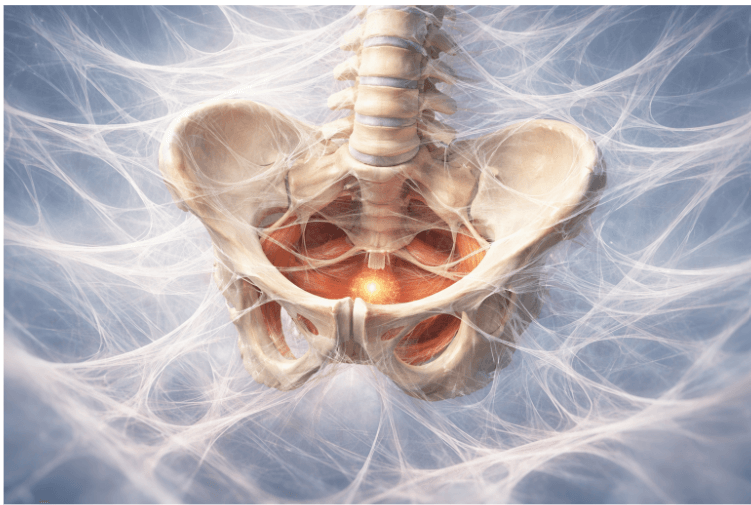
The pelvic floor isn’t one muscle. It’s a layered group of muscles and connective tissue that form the base of your deep core canister—a pressure system made up of the diaphragm (top), pelvic floor (bottom), transverse abdominis (front and sides), and multifidus (back).
These structures work together to stabilize the spine, regulate intra‑abdominal pressure, and coordinate breath with movement.
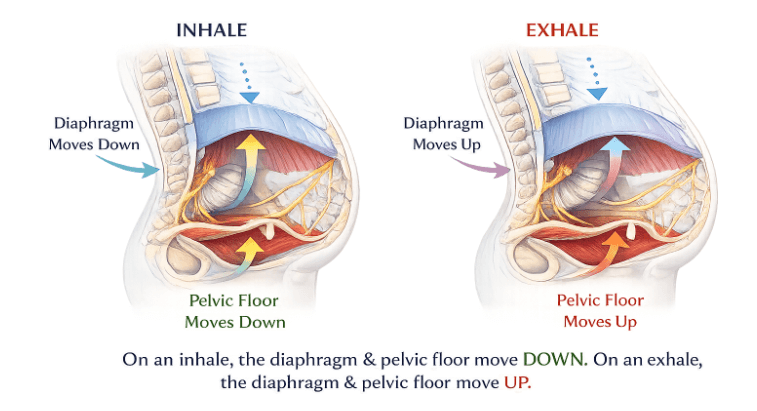
When you inhale, the diaphragm descends and the pelvic floor lengthens slightly to accommodate the pressure shift.
On exhale, both gently lift and recoil, creating a rhythmic co‑regulation between breath and pelvic support. Research on breath and the pelvic floor show that coordination of diaphragm–pelvic floor synergy is essential for continence, spinal stability, and efficient breathing patterns.
Here’s something that confuses most of my students, and is important to break down and look at before we move on further.
On an inhale, your diaphragm contracts and moves down. That downward movement increases pressure in the abdomen, so the pelvic floor responds by softening/lengthening and moving slightly down as well (think: “receiving” the pressure).
On an exhale, your diaphragm relaxes and rises up, and the pelvic floor recoils and gently contracts, lifting back up like a trampoline returning to center.
So yes: the movements mirror each other (down on inhale, up on exhale), but the pelvic floor is generally relaxing on inhale and contracting on exhale, while the diaphragm is doing the opposite (contracting on inhale, relaxing on exhale).
In my podcast on the impact of stress on hip & pelvic health, which also inspired a blog on my favorite advanced pelvic floor breath, pelvic floor PT Dr. Brianne Grogan explains it like this: pelvic floor fascia links into the hip rotators, then into the iliopsoas/hip flexors, and continues up to the breathing diaphragm.
So when we’re talking about your “pelvic floor,” we’re also talking about:
- your hips
- your breath mechanics
- your abdominal pressure system
- your threat response patterns
- your fascia network
Emotionally, this deep core canister mirrors your nervous system tone.
When stress or fear triggers shallow breathing, the diaphragm stops moving freely, and the pelvic floor often mirrors that by tightening or bracing. Over time, this creates emotional patterning—your body literally “holds its breath” and “holds its ground” at the same time.
That’s why the somatic pelvic floor approach matters: you can’t separate pelvic tone from nervous system tone.
Medical references describe pelvic floor dysfunction as a broad constellation of symptoms that can involve
- increased activity (hypertonicity)
- decreased activity (hypotonicity)
- or poor coordination
Don’t worry, we’ll explore each one.
Tight Pelvic Floors (Hypertonic): The Hidden Epidemic No One Talks About
A tight pelvic floor (also called a hypertonic pelvic floor) means the muscles are in a state of increased tone or contraction and have difficulty relaxing.
In clinical terms, hypertonicity refers to persistently elevated resting muscle activity in the pelvic floor, which can interfere with normal bladder, bowel, and sexual function.
This matters because a pelvic floor that can’t relax can’t do its job well. When the muscles remain shortened, blood flow, nerve signaling, and pressure regulation are disrupted, often leading to pain and dysfunction.
Common symptoms of a tight pelvic floor (hypertonic pelvic floor)
These can include:
- pelvic floor pain or pressure
- pain with penetration / painful sex (dyspareunia)
- vulvar burning or irritation (vulvodynia)
- pain while urinating
- urinary urgency or frequent urination
- difficulty starting a urine stream (urinary hesitancy)
- dysfunctional voiding or incomplete emptying
- constipation or difficulty fully emptying stool
- pelvic muscles that feel “clenched” or “stuck”
- low back pain and hip tightness
- a sore pelvic floor after exercise or stress
- “my pelvic floor won’t relax” (the most honest symptom description ever)
Hypertonic pelvic floor symptoms often overlap with chronic pelvic pain conditions such as dyspareunia, vulvodynia, and dysfunctional voiding. But don’t worry, you can find relief, these conditions can be treated effectively with pelvic floor physical therapy and down-training.
Why it happens
Hypertonicity is often linked to stress, perfectionism, and trauma patterns.
Chronic stress can keep the nervous system in a state of vigilance, leading to unconscious clenching of the pelvic muscles—similar to how shoulders rise toward the ears under tension.
Perfectionistic or “holding it together” tendencies can reinforce this bracing pattern, while unresolved trauma (including sexual, birth, or medical trauma) can condition the body to maintain protective guarding in the pelvic region. Over time, this creates a feedback loop of tension, pain, and further guarding.
“We all know our shoulders get tense when we’re stressed… but we don’t think about that happening in our pelvic floor.”
Mula bandha is not the only way to work with the pelvic floor in yoga. Unfreeze with me by practicing Somatic Exercises to Reduce Cortisol & Get Out of Freeze Response.
Weak Pelvic Floors (Hypotonic): When Strengthening Actually Helps
A weak pelvic floor—also called a hypotonic pelvic floor—refers to muscles that have decreased tone and reduced resting tension, meaning they cannot generate or sustain enough force to support the pelvic organs or maintain continence.
Hypotonicity can develop after pregnancy, childbirth, hormonal changes, or prolonged inactivity.
Common weak pelvic floor (hypotonic) symptoms
These can include:
- leaking urine when coughing, sneezing, or jumping (stress incontinence)
- fecal incontinence (leaking stool)
- sensations of heaviness or pressure in the pelvis
- pelvic organ prolapse (a feeling of bulging or “something dropping”)
- difficulty maintaining posture or core stability
Dr. Grogan describes prolapse sensations as feeling like a bulge, even “like a golf ball in your vagina.”
Science note: Pelvic floor muscle training (PFMT) is one of the most evidence-based treatments for urinary incontinence. A Cochrane review found that women performing PFMT were significantly more likely to report cure or improvement compared with controls, confirming that targeted strengthening can restore continence and pelvic support.
So yes: strength matters. Pelvic floor strength matters. Strengthen your pelvic floor with me in this class – no you do not have to be pregnant like I am in the video to benefit!
But here’s the trap:
If your pelvic floor is already tight, strengthening can backfire.
Why Most Women Get Misdiagnosed
Because the default public narrative is:
- “Leaking? Weak pelvic floor.”
- “Pelvic pain? Weak pelvic floor.”
- “Postpartum? Weak pelvic floor.”
- “Sex pain? Weak pelvic floor.”
Then the internet says: Do Kegels.
Kegels aren’t “bad” per se. They’re just not always the right first step.
Here’s where the system breaks down:
- There’s an overfocus on Kegels as the universal fix, even when the issue isn’t weakness.
- Most people are never assessed for tone—no one checks whether the muscles are already tight before prescribing strengthening.
- Hypertonic patients get treated as hypotonic, meaning those with overactive pelvic floors are told to “tighten more,” which only worsens symptoms.
- Trauma isn’t accounted for, even though the pelvic floor often holds protective tension from past experiences.
- And there’s a medical bias toward “strengthen everything”, a cultural reflex that equates effort with healing.
If you do Kegels and your symptoms get worse, it can indicate too much tension or poor technique.
This is the misdiagnosis loop:
- tight pelvic floor symptoms get labeled as weakness
- “strengthening” increases tone even more
- pain/urgency/constipation increase
- woman feels broken
- she tries harder
That’s not healing. That’s bracing.
Trauma & the Pelvic Floor: Your Body Trying to Protect You
This is the part most often avoided.
The pelvic floor is not only mechanical. It’s also deeply protective.
In my podcast interview, Dr. Grogan references a study that measured muscle response while women watched emotionally provocative film clips. The pelvic floor reacted more and faster than the upper trapezius muscles during anxiety- and threat-inducing clips.
That means your pelvic floor can tense before your conscious mind even has a chance to narrate what’s happening. Isn’t that crazy!
Why trauma can show up as pelvic floor tightness
Trauma (big “T” or little “t”) can train the body toward:
- clenching (protection)
- bracing (control)
- freezing (immobility)
- hypervigilance (constant readiness)
And yes, this can include sexual trauma, birth trauma, medical trauma, or chronic relational stress.
These experiences often imprint through the autonomic nervous system, where the body’s fight, flight, or freeze responses become patterned into muscle tone and breath. It’s essential to understand these core trauma responses and how to repattern by learning the language of your animal body.
I suggest chapters 2 and 3 in my book Healing with Somatic Yoga: A 6-Week Journey to Release Emotions, Rewire Your Nervous System, and Reclaim Your Body.
Research on trauma physiology shows that the freeze response—a parasympathetic-dominant state—can lead to muscular immobility and fascial guarding, particularly in the psoas and pelvic floor, which act as key stabilizers and emotional “brakes” during threat.
Over time, chronic stress can keep these reflexes switched on.
The fascia surrounding the pelvic organs and hips may remain shortened or “armored,” limiting circulation and sensation. This is sometimes called fascia guarding—a protective holding pattern that mirrors the body’s unresolved startle or freeze reflex. Hint hint —this is why you always hear yoga teachers talking about emotional release in the hips.
The pelvic floor is also wired into pelvic autonomic reflexes—automatic responses that regulate urination, defecation, and sexual arousal.
When the nervous system perceives danger, these reflexes can shift instantly: muscles tighten, sphincters close, and blood flow changes.
It’s not a conscious choice; it’s a survival reflex.
So when we talk about trauma and the pelvis, we’re really talking about the somatic story of protection.
The pelvic floor is part of your threat response system—a living interface between your emotions, your fascia, and your physiology. When safety returns and the body learns to move and breathe again, those protective patterns can finally unwind.
We nerd out on all things fascia and anatomy in my 200-Hour Yoga Teacher Training.
Somatic Patterns That Create Pelvic Floor Holding
Let’s be blunt: we’re taught to be ashamed of this part of our body.
The pelvic area is associated with pee, poop, blood, sex, and trauma, and many people disconnect from it for that reason.
This area becomes a “second class citizen” in our awareness, while shoulder pain and headaches feel socially acceptable to discuss.
“Maybe we’re all yapping about the hips because it’s the closest we can get… without getting too close to where poop and sex happens.”
In somatic terms, pelvic floor tension can also be fed by:
- clenching for safety (a subconscious “armor” response)
- habitually sucking in the belly
- chronic glute gripping
- “tuck your tailbone” cueing that over-stabilizes
- anxiety-driven breath holding
- perfectionism (“I must hold it together”)
- posture habits that keep the ribs thrust forward or the pelvis tucked under
- shame patterns that make us pull away from sensation in this area
All of this can create pelvic muscle strain and chronic pelvic guarding, and it’s not just muscular—it’s fascial.
The fascia network that wraps through the pelvis, hips, and abdomen is continuous with the diaphragm and even the soles of the feet.
Research on fascia and emotional holding suggests that this connective tissue can store tension patterns through its piezoelectric properties—tiny electrical charges that respond to mechanical stress—linking physical bracing with emotional states.
When we soften and move, we’re not only releasing muscle tone but also recalibrating this fascial communication network.
Use this class to do exactly that: 30 Min Somatic Yoga Flow through Somatic Movement for Hips, Lower Back, Sacral Chakra
How to Tell If Your Pelvic Floor Is Tight or Weak (At Home Test)
A pelvic floor PT assessment is the gold standard. But here are practical clues you can use now.
Signs you may be more on the “weak” side
- leaking urine with impact (running, jumping, coughing)
- fecal incontinence
- heaviness/bulging/prolapse sensations
Signs you may be more on the “tight” side
- painful sex
- difficulty starting urine stream
- urinary frequency/urgency
- constipation or straining
- pelvic floor pain or burning
- symptoms worsen with Kegels
A very “nuts and bolts” self-test
If you do Kegels and you feel:
- increased pain
- more urgency
- more tension
- worse symptoms overall
That’s a sign you may need pelvic floor relaxation and down-training before strengthening.
Also: if constipation is a chronic theme, pelvic floor tension may be part of the story.
And if you look back and notice your symptoms began during a period of intense stress or upheaval, that mind-body correlation matters.
Why Kegels Make Tight Pelvic Floors Worse
Kegels are a contraction pattern, and when they’re performed on a muscle that’s already over-recruited—meaning it’s chronically engaged and unable to fully relax—they can amplify dysfunction rather than resolve it.
Over-recruitment happens when the pelvic floor muscles stay partially contracted even at rest. This constant tension limits blood flow, restricts range of motion, and keeps the nervous system in a low-level “on” state. When you add more contractions (like repetitive Kegels) to a muscle that can’t release, you reinforce the holding pattern instead of restoring balance.
It’s like a bicep that’s so tight it can’t go through its full range of motion—trying to strengthen it further only deepens the restriction.
In somatic terms, you can’t “effort” your way out of bracing; the body needs to relearn how to let go before it can safely engage.
Science note: Clinical research supports this. Studies have shown that excessive or poorly guided Kegel exercises can worsen pelvic floor hypertonicity and pain, particularly in women with overactive pelvic floor disorders or chronic pelvic pain syndromes. These findings highlight that strengthening without relaxation can perpetuate dysfunction rather than resolve it.
Somatic Healing Masterclass: Rewire Trauma, Reclaim Your Intuition (usually $67) FREE👇

Can My Pelvic Floor Be Both Weak and Tight? (YES — and It’s Extremely Common)
This is one of the biggest reasons women get misdiagnosed, because on the surface it looks like “weakness”… but underneath it’s often protective tension layered over fatigue.
1. Here’s the Most Common Pattern in Women
Here’s what “weak + tight” usually means in real life:
- Chronic gripping = tight. The pelvic floor (often the more superficial layers) stays subtly contracted most of the day, like a fist that never fully opens.
- Underfunctioning deeper layers = weak. The deeper support system can’t coordinate and recruit well, because the baseline tone is already too high.
- Stress + trauma + postpartum = protective tension. Your nervous system learns to guard this area after pain, uncertainty, shame, birth/pregnancy, or prolonged stress.
Dr. Brianne Grogan noticed this shift firsthand during the pandemic. She talked about how many people’s pelvic floor strengthening routines stopped working because their pelvic areas were already tight from uncertainty and stress — that’s when she switched up her programs, prioritizing release first, then strength.
2. Why “Weak + Tight” Leads to Misdiagnosis
Because the symptoms overlap.
- You might leak urine and have pelvic floor pain.
- You might feel “weak” during exercise and feel clenched at rest.
- You might have prolapse symptoms and difficulty relaxing enough to poop without straining.
So the system does what it’s trained to do: it treats “weakness” and skips assessing tone.
That’s where blanket Kegel advice can make things worse: if the pelvic floor is already bracing, more contraction piles onto the bracing.
3. The Golden Rule: Release First, THEN Strengthen
This is the order that changes everything:
- Down-train first.
Teach the pelvic floor and nervous system how to soften. - Soften fascia and restore range.
If the tissue can’t lengthen, it can’t function well. - Restore breath–diaphragm coordination.
When the diaphragm moves, the pelvic floor responds. - Then build strength safely.
Strength is helpful when it’s layered onto a system that can also relax.
If you suspect you’re both tight and weak, your job is not to “try harder.”
Your job is to change the baseline first.
Start here:
- Somatic softening: breath, slow movement, gentle pelvic circles, hip mobility without forcing.
- Nervous system regulation: anything that helps your body feel safe enough to stop bracing.
- After release → functional strengthening: once you can relax, strength work actually lands.
A helpful cue from Dr. Grogan that brings this into the body fast is:
“Inhale to expand, exhale to engage.”
And yes, we’re going fully clinical here because it helps:
Lie down and place two fingers gently on the perineum (between the vagina and anus). Notice the pelvic floor subtly descend/soften on inhale and lift/recoil on exhale.
That’s biofeedback you can do at home.
If you want a stronger external “feedback tool,” I like to use a malleable meditation cushion to feel pressure changes more clearly.

When to See a Pelvic Floor PT?
If you have any of the following, don’t white-knuckle it alone:
- persistent pelvic floor pain (burning, aching, sharp pain)
- pain with sex or penetration
- urinary urgency/frequency or difficulty starting urine stream
- constipation with straining
- prolapse symptoms (bulging/heaviness)
- symptoms that worsen with Kegels
- a trauma history (sexual trauma, birth trauma, medical trauma) + pelvic symptoms
A pelvic floor PT can assess tone and coordination directly (sometimes internally, vaginally or rectally) and help you down-train before you strengthen.
Somatic Pelvic Floor Healing: Bottom-Up, Nervous-System-First
If you’re used to approaching your body like a project, somatic healing can feel almost offensive at first — because it’s not about “fixing.”
It’s about listening, softening, and re-teaching your nervous system that it doesn’t have to brace in order to survive.
Here are a few bottom-up tools that consistently help with pelvic floor relaxation, pelvic floor dysfunction patterns, and “pelvic floor won’t relax” symptoms:
1) Move the hips slowly enough to feel something change
This somatic sacral flow class is perfect when pelvic floor tension is connected to hips, low back, and that “sacral chakra / bracing” vibe.
2) Regulate first, then try to “do the work”
If stored stress or trauma is part of the picture, this class supports vagus nerve health and downshifting out of bracing.
3) Strengthen in a way that still honors relaxation
This pelvic floor strengthening routine is especially useful once you’ve started to regain range and breath coordination (and no, you don’t have to be pregnant to benefit).
4) Go slower than you think you need to
Dr. Grogan shares an anecdote that is a perfect expression of how somatic movement can work: doing hip circles so slowly that emotion rose up unexpectedly — and the key instruction was to slow down even more.
“Go 20% slower than you think is slow.”
That’s not just a cute line. It’s a nervous system intervention.
Because your pelvic floor doesn’t soften through force.
It softens through safety.
In my own somatic yoga approach, the same principles apply — but we make them tangible through specific embodied tools:
- Breath as a dial: learning to modulate tone and release through the breath, using it as a volume knob for the nervous system.
- Gentle swaying, circles, and undulation: rhythmic movement that coaxes the fascia and pelvic diaphragm to respond rather than resist.
- Sound + vibration: humming, sighing, and toning to stimulate the vagus nerve and deepen pelvic floor coordination.
- Slow fascia release: micro-movements and sustained holds that invite the tissue to melt instead of stretch.
- Three-diaphragm model: integrating the vocal, respiratory, and pelvic diaphragms so the whole body breathes as one system.
[SCIENCE NOTE: Research shows that vagus nerve stimulation and diaphragmatic breathing improve pelvic floor coordination and autonomic regulation, supporting both relaxation and strength.]
You can explore these exercises and learn how to repattern and communicate with your body in my new book, Healing with Somatic Yoga: A 6-Week Journey to Release Emotions, Rewire Your Nervous System, and Reclaim Your Body— available now on Amazon.
These are also the foundations I teach in my Somatic Yoga Teaching Training — 75-Hour Home Study Course.
If you’re ready to embody this work, deepen your understanding of the nervous system, and guide others through true bottom-up healing, join me inside the training.
Your body — and your students — will thank you.
Next Steps
- Take a deep dive into embodiment and somatic yoga with my Somatic Yoga certification program.
- If you’re interested in practical kriya yoga as a way to improve your daily life and relationships, check out my Yoga for Self Mastery course.

YOU MIGHT ALSO LIKE
- Somatic Yoga vs Somatic Therapy: What’s the Difference?
- 8 Top Somatic Yoga Books to Regulate Your Nervous System
- 5 Best Somatic Yoga Apps for Nervous System Regulation
- Top Somatic Coaching Programs And How To Choose One
- Somatic Yoga Workshop Ideas for Teachers
- Somatic Yoga for Cortisol Detox: A Gentle Path to Stress Relief and Nervous System Healing
- Gentle Somatic Yoga: Heal Chronic Pain, Release Trauma, and Reclaim Your Bod
- Somatic Meditation: A Body-Based Approach to Healing Stress, Anxiety, and Trauma
- Advanced Pelvic Floor Breathing: A Somatic Approach to Healing
- Somatic Yoga For Yoga Teachers: Everything You Need to Know in 10 Steps
- How Somatic Shaking Can Release Tension and Reset Your Nervous System
- Discover Somatic Pilates: Enhance Your Body Awareness and Flexibility
- Kundalini for Feminine Energy: Ignite Your Creative Power and Passion
- 6 Effective Somatic Yoga for Neck and Shoulders
- How to Teach Somatic Yoga: A Practical Guide for Instructors